Definition
Müllerian agenesis, also known as Müllerian aplasia, Mayer-Rokitansky-Küster-Hauser syndrome, or vaginal agenesis, is a developmental disorder during the fetal stage where the vaginal canal, uterus, or both fail to develop. This condition occurs in 1 out of 4,500–5,000 females. Müllerian agenesis is typically identified during an examination prompted by complaints of never having menstruated.
Müllerian agenesis is one of the most common causes of amenorrhea (absence of menstruation) in females who experience normal breast and body hair development.
Müllerian agenesis is classified into two types:
- Type I (isolated uterovaginal aplasia): abnormalities only in the uterus and vagina.
- Type II: abnormalities also found outside the reproductive tract, such as in the kidneys, bones, ears, or heart.
Causes
The exact cause of Müllerian agenesis is unknown. However, it occurs when the Müllerian duct fails to develop properly during the first 20 weeks of pregnancy.
Normally, the lower part of this duct develops into the uterus and vagina, while the upper part becomes the ovaries. Disruption in the development of the Müllerian duct results in the absence of all or part of the vagina, uterus, or both.
Risk Factor
Experts estimate that certain genetic and environmental factors contribute to the occurrence of Müllerian agenesis. These factors may include medication use during pregnancy, certain illnesses, or other factors.
If there is a history of sexual differentiation disorders in your family, you may be at risk of giving birth to a baby with Müllerian agenesis.
Symptoms
Symptoms that may be found in Müllerian agenesis include:
- Absence of menstruation. However, if part of the uterus develops, monthly cramps or prolonged abdominal pain may occur
- Normal height
- Normal breast development
- Normal body hair
- Normal external genitalia
- A vagina that may appear as a small dimple or a longer vagina without a cervix at the top
Müllerian agenesis can also be associated with other issues, such as:
- Kidney and urinary tract developmental disorders
- Spinal, rib, and wrist bone development disorders
- Hearing disorder
- Other congenital conditions involving the heart, gastrointestinal tract, and limb growth
Diagnosis
Müllerian agenesis is often identified during puberty when a female does not experience her first menstruation. To evaluate females with abnormalities in the vagina, cervix, or uterus, the doctor will first conduct a medical interview, physical examination, and then laboratory tests.
Medical Interview
The doctor will ask about the current complaints, whether menstruation has occurred for the first time, whether there are similar complaints in the family, and any additional complaints. The first menstruation, also known as menarche, usually occurs between the ages of 10 and 16 years and is considered late if it occurs after age 15.
You can read more about the first menstrual period here: Menarche - Definition, Cause, Symptom, And Treatment
Physical Examination
During a physical examination, vital signs will be checked, including blood pressure, respiratory rate, body temperature, and pulse rate. If delayed puberty is found in a woman who has not menstruated, FSH hormone levels and genetic testing may be conducted. The most common cause of amenorrhea and delayed puberty is Turner syndrome.
Diagnostic Examinations
Laboratory Tests
- Testosterone levels
- FSH (follicle-stimulating hormone) levels
- Genetic testing (karyotyping)
Radiological Examinations
- Abdominal, vaginal, and rectal ultrasound to assess for residual uterus
- Magnetic Resonance Imaging (MRI) to visualize the structure of the remaining reproductive tract, found in 90% of Müllerian agenesis patients
During examinations, a very short vaginal canal may be found, which could be just a dimple below the urethral opening. Residual uterus tissue in the middle of the pelvic cavity or uterine horns with or without a uterine cavity may be found in the pelvis. Since the ovaries develop differently during the fetal stage, their structure and function usually remain normal, although they may be in an abnormal location.
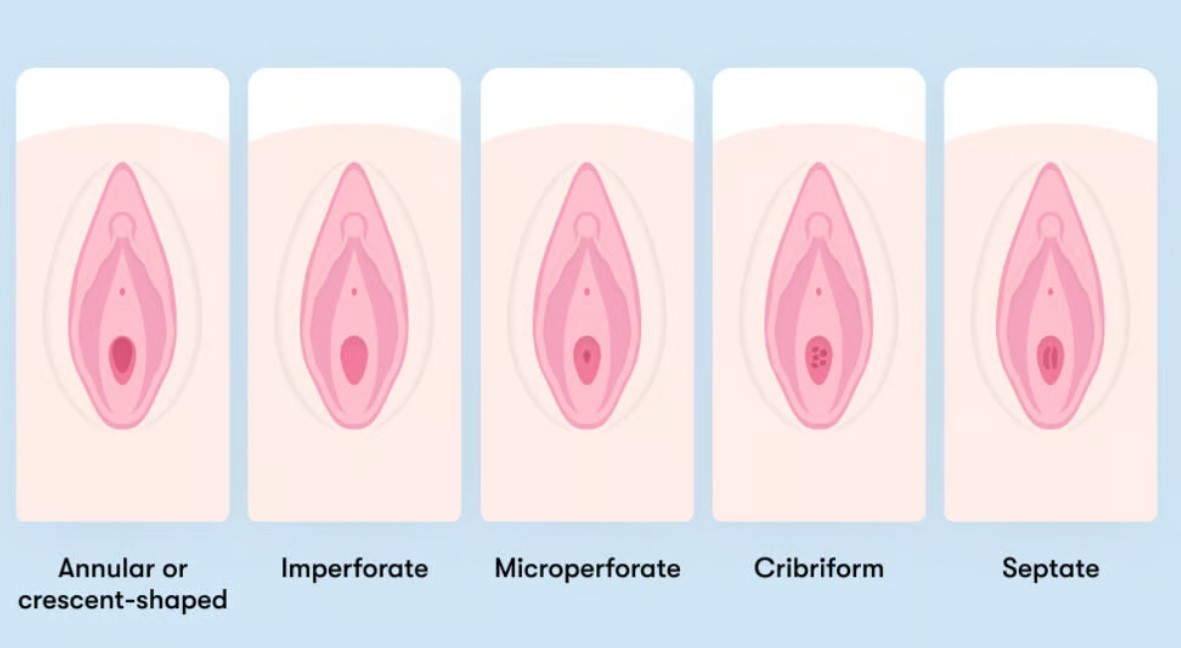
Doctors will conduct other tests to rule out other abnormalities, such as an imperforate hymen or other vaginal and cervical tract anomalies. The doctor will examine the hymen with an instrument to view the inside of the vagina under magnification. However, this examination may not sufficiently distinguish Müllerian agenesis as it can resemble other conditions. Therefore, pelvic radiology examinations may be conducted for further evaluation of internal structures.
One of the conditions most commonly confused with Müllerian agenesis is androgen insensitivity syndrome. Both conditions cause amenorrhea, a short vagina, and the absence of a cervix. To differentiate between these conditions, blood testosterone levels can be measured, followed by genetic testing.
Evaluation of other congenital abnormalities associated with Müllerian agenesis is important because about 53% of Müllerian agenesis patients have other congenital abnormalities, particularly in the urinary tract. Many studies have confirmed that the incidence of kidney abnormalities in Müllerian agenesis patients is around 27–29%. Therefore, kidney ultrasound is usually performed on all patients. Bone abnormalities (such as scoliosis, spinal curvature disorders, and wrist development disorders) are reported to occur in 8–32% of patients. Spinal X-rays can show bone abnormalities even in asymptomatic individuals.
Management
Non-surgical vaginal elongation (dilation) is the first choice of therapy. This procedure involves using a tube-like device that stretches the vagina when used over a certain period. With proper counseling and emotional support, nearly all patients (90–96%) can achieve a functional vagina with this procedure. This procedure is preferred because it is safer and more affordable than surgery. Surgery is usually only performed in rare cases where dilation is unsuccessful, or the patient requests surgery after a thorough discussion with the doctor and family.
This therapy allows patients to engage in sexual activity. Women with Müllerian agenesis who are sexually active still have a risk of sexually transmitted infections (STIs) and should use condoms during intercourse. Additionally, STI screening should still be conducted.
Future childcare options can also be discussed. These options include adoption and pregnancy surrogacy. Gestational surrogacy involves a surrogate mother carrying the child. Assisted reproductive techniques with gestational carriers have proven successful for women with Müllerian agenesis.
All Müllerian agenesis patients are offered counseling and participation in peer support groups consisting of young women with the same diagnosis to cope with the psychological impact. Parents or caregivers can also benefit from counseling to manage their feelings, enabling them to better support their child.
Complications
In Müllerian agenesis, there may be an active uterine lining without a cervix and upper vagina. It can cause menstrual blood flow blockage, leading to retrograde menstruation, where the blood flows backward, causing endometriosis. This can result in pelvic pain.
Müllerian agenesis has a significant psychological impact. Many patients experience anxiety and depression, question their femininity, and grieve over infertility. Patients may also struggle to share their condition with family, friends, and partners.
Prevention
Müllerian agenesis is a congenital condition (birth defect). This means the condition is present at birth, even while the baby is developing in the womb. Therefore, there is no way to prevent it.
When to See a Doctor?
If you have not menstruated by the age of 15, you should consult a doctor immediately.
Looking for more information about other diseases? Click here!
- dr. Monica Salim
Müllerian agenesis: Diagnosis, management, and treatment (2020) ACOG. Available at: https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2018/01/mullerian-agenesis-diagnosis-management-and-treatment (Accessed: November 4, 2022).
Vaginal agenesis - symptoms and causes - mayo clinic (2022). Available at: https://www.mayoclinic.org/diseases-conditions/vaginal-agenesis/symptoms-causes/syc-20355737 (Accessed: November 4, 2022).
Mayer-Rokitansky-Küster-Hauser Syndrome: Medlineplus Genetics (no date) MedlinePlus. U.S. National Library of Medicine. Available at: https://medlineplus.gov/genetics/condition/mayer-rokitansky-kuster-hauser-syndrome/#inheritance (Accessed: November 4, 2022).
WebMD. 2021. Using a Surrogate Mother: What You Need to Know. Available from: https://www.webmd.com/infertility-and-reproduction/guide/using-surrogate-mother