Definisi
Angina pektoris merupakan sebuah sensasi tertekan atau nyeri pada dada, yang disertai dengan rasa cemas. Kondisi ini terjadi ketika otot-otot jantung kekurangan oksigen akibat penurunan aliran darah. Angina pektoris pada anak jarang sekali terjadi, namun seringkali menjadi kekhawatiran orang tua ketika anak mengalami nyeri dada. Nyeri dada pada anak seringkali memiliki penyebab yang berbeda daripada orang dewasa.
Penyebab
Pada anak, nyeri dada dapat disebabkan oleh berbagai hal. Penyebab ini dapat berasal dari otot dan tulang, paru-paru, atau idiopatik (atau tidak diketahui asalnya karena tidak ada masalah yang ditemukan).
Masalah Otot dan Tulang
Nyeri dada akibat masalah otot dan tulang terjadi apabila ada masalah pada otot dinding dada. Pada satu penelitian, gangguan pada otot dan tulang merupakan penyebab tersering dari nyeri dada (37,1%).
Masalah Paru
Sementara itu, nyeri dada akibat masalah paru dapat disebabkan oleh asma dan pneumonia (infeksi pada paru-paru).
Penyakit Jantung
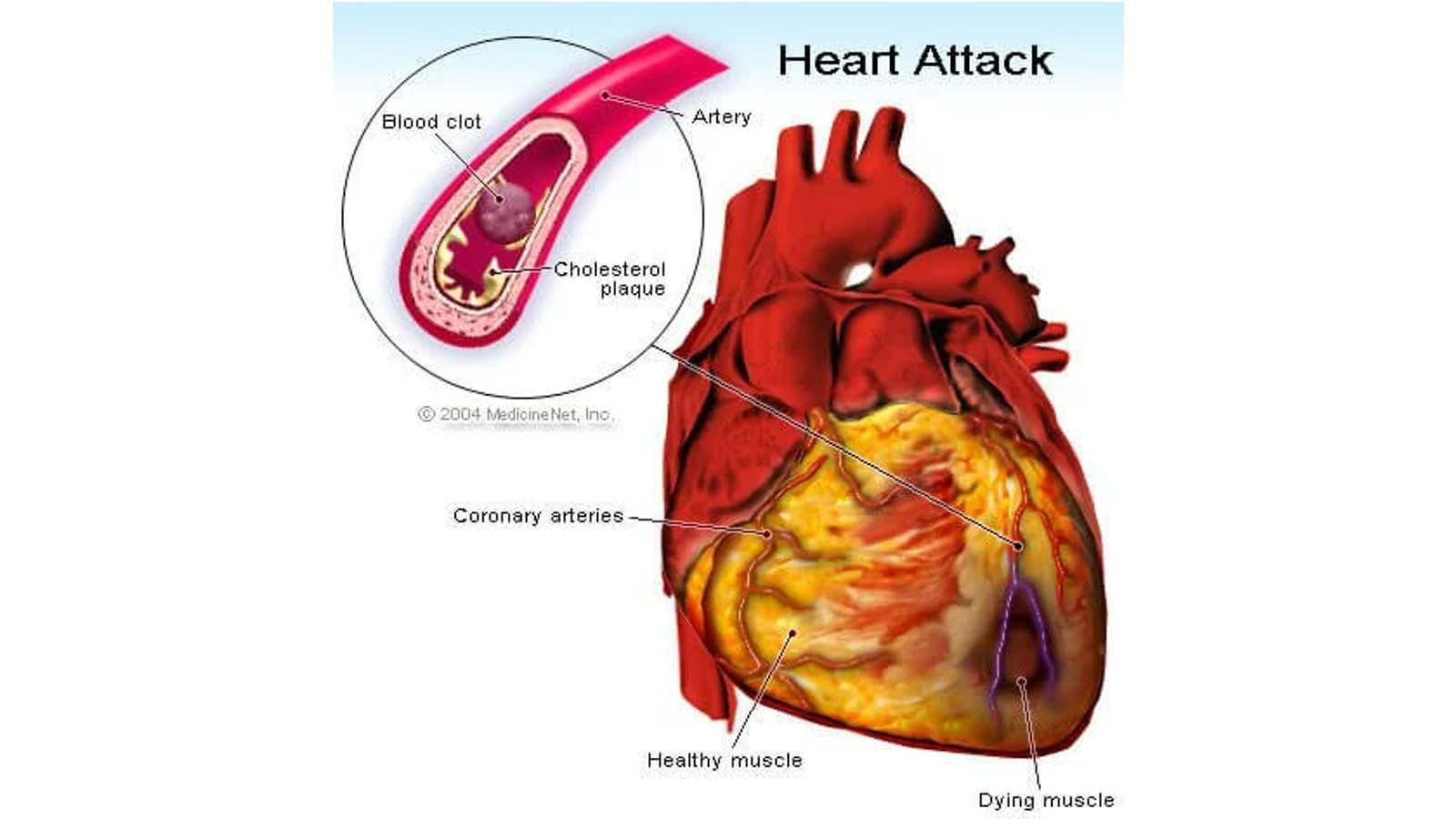
Nyeri dada akibat penyakit jantung jarang terjadi pada anak-anak. Nyeri dada akibat penyakit jantung pada anak dapat disebabkan oleh peradangan pada selaput jantung (perikarditis) dan angina pektoris yang disebabkan oleh kekurangan oksigen pada otot-otot jantung.
Terdapat beberapa kelainan pembuluh nadi bawaan yang dapat menyebabkan kadar oksigen di pembuluh nadi rendah, sehingga kebutuhan oksigen otot-otot jantung tidak terpenuhi. Pada gangguan lainnya, otot-otot jantung membutuhkan oksigen lebih banyak karena otot-otot tersebut menebal, yang disebut sebagai kardiomiopati. Pada kelainan lainnya, terdapat sumbatan pembuluh darah dari jantung sehingga otot-otot jantung menebal karena dipaksa untuk bekerja lebih keras.
Penyempitan pembuluh nadi karena pembentukan plak lemak, seperti layaknya orang dewasa merupakan kondisi yang sangat jarang terjadi pada anak. Bila terjadi penurunan aliran darah akibat penyempitan pembuluh nadi, biasanya merupakan akibat dari penyakit yang melibatkan pembuluh nadi, seperti:
- Penyakit Kawasaki
- Tingginya kadar kolesterol bawaan
- Kelainan bawaan atau gangguan sejak lahir pada pembuluh nadi koroner anak
- Komplikasi yang timbul pada pembuluh nadi koroner karena penyakit jantung bawaan anak
Faktor Risiko
Faktor risiko yang meningkatkan kejadian angina pektoris pada anak sangat tergantung dari kondisi yang ada. Misalnya pada penyakit Kawasaki, kemunculan penyakit dipengaruhi oleh usia dan paling berisiko tinggi terjadi pada anak berusia di bawah 5 tahun. Selain itu, penyakit ini lebih sering terjadi pada anak laki-laki daripada anak perempuan. Tidak hanya itu, anak dari ras Asia Pasifik, misalnya keturunan Jepang atau Korea, lebih rentan terhadap penyakit ini. Penyakit tersebut juga lebih banyak muncul pada musim-musim tertentu. Di Amerika Utara, penyakit ini lebih sering terjadi pada akhir musim dingin dan awal musim semi.
Gejala
Angina pektoris pada anak biasanya muncul berupa rasa nyeri pada dada yang dapat menjalar ke lengan kiri atau ke rahang. Biasanya, nyeri dideskripsikan seperti rasa tertindih beban yang sangat berat. Pada angina pektoris, napas dapat terasa berat, namun bernapas tidak memperparah rasa nyeri. Nyeri pada angina pektoris juga biasanya tumpul dan sulit untuk ditunjuk secara langsung. Rasa nyeri tersebut juga bukan seperti tertusuk atau tertikam. Biasanya, rasa nyeri ini berlangsung kurang dari 5 menit. Nyeri ini biasanya terjadi saat melakukan aktivitas yang menaikkan kerja jantung, misalnya berolahraga. Namun, gejala akan berkurang atau bahkan hilang saat beristirahat atau mengonsumsi obat tertentu.
Pada anak-anak, nyeri angina bisa muncul tidak dengan gambaran khas seperti di atas, namun dengan gejala tidak spesifik seperti:
- Anak mudah marah atau gelisah karena sensasi angina yang dirasakannya
- Mual dan muntah
- Nyeri perut
- Pingsan atau sinkop
- Kejang
- Henti jantung mendadak
Diagnosis
Diagnosis angina pektoris pada anak mirip dengan orang dewasa. Dokter akan menanyakan riwayat gejala nyeri dada angina sebelumnya dan bila terdapat riwayat penyakit jantung bawaan. Selanjutnya akan dilakukan beberapa pemeriksaan. Pemeriksaan ini dapat berupa:
1. EKG (Elektrokardiografi)
EKG merupakan sebuah pemeriksaan yang berfungsi untuk mengamati aliran listrik jantung. Pasien akan dipasangi beberapa patch di dada, pergelangan tangan, dan pergelangan kaki, dan dari sana aliran listrik jantung dapat terdeteksi.
2. Ekokardiografi
Pemeriksaan ekokardiografi adalah pemeriksaan ultrasonografi pada jantung, yang menggunakan gelombang suara untuk melihat aliran darah pada jantung.
3. Stress Test
Stress test merupakan tes untuk menguji kerja jantung baik sebelum dan sesudah aktivitas fisik atau pemberian obat. Aktivitas fisik yang dilakukan dapat berupa berlari di atas treadmill atau bersepeda, sementara obat-obatan yang diberikan berfungsi untuk memacu kerja jantung, selayaknya anak melakukan aktivitas fisik.
4. Rontgen Dada
Selain pemeriksaan di atas, dokter mungkin akan menyarankan anak Anda untuk menjalankan pemeriksaan rontgen dada. Rontgen dada dapat dilakukan untuk melihat bentuk jantung, paru, serta organ lainnya pada rongga dada.
Tata Laksana
Terapi angina pektoris pada anak tergantung dari penyebabnya. Secara umum, terapi dapat bertujuan untuk menurunkan kebutuhan oksigen otot-otot jantung atau untuk meningkatkan aliran darah ke otot-otot jantung. Salah satu cara yang dapat dilakukan adalah mengurangi aktivitas fisik untuk meningkatkan kondisi anak. Namun, cara ini sangat terbatas. Obat-obatan dapat pula diberikan, terutama obat golongan nitrat. Nitrat berfungsi untuk meningkatkan aliran darah ke jantung, serta menurunkan beban kerja jantung dengan memperlebar pembuluh darah dan menurunkan tekanan darah.
Angioplasti atau Coronary Artery Bypass Surgery (CABG)
Pada kondisi pembuluh nadi yang lebih parah, tindakan seperti pembedahan mungkin akan dilakukan. Sebagian besar anak dengan kelainan pembuluh nadi bisa disarankan untuk menjalani tindakan tertentu. Tindakan ini dapat berupa angioplasti atau coronary artery bypass surgery (CABG). Angioplasti merupakan sebuah tindakan yang bukan pembedahan, bertujuan untuk membuka pembuluh nadi pada jantung agar aliran darah kembali lancar. Pembukaan pembuluh nadi ini menggunakan balon atau stent/ring yang dimasukkan lewat selang yang masuk ke pembuluh nadi jantung.
Sementara itu, CABG merupakan pembedahan yang dilakukan dengan mengambil pembuluh darah di tempat lainnya (misalnya pada tungkai) yang kemudian dipasang di pembuluh nadi. Pembuluh darah dari tempat lainnya ini akan berfungsi sebagai jalan pintas (bypass) agar aliran darah ke otot-otot jantung tetap baik.
Terapi Obat
Jika angina pektoris disebabkan oleh penumpukan kolesterol pada pembuluh nadi, Anda akan bekerja sama dengan dokter untuk melakukan terapi diet untuk mengontrol kadar kolesterol dan lemak pada anak Anda. Dokter juga dapat memberikan obat-obatan untuk menurunkan kadar kolesterol dan lemak pada darah.
Sementara itu, jika anak Anda terkena penyakit Kawasaki, dokter akan menangani demam dan peradangan untuk mencegah kerusakan jantung. Tata laksana yang dapat diberikan berupa gamma globulin dan aspirin. Gamma globulin merupakan komponen kekebalan tubuh yang dapat menurunkan peradangan pada pembuluh darah. Sementara itu, aspirin dapat diberikan untuk menurunkan rasa nyeri, peradangan pada sendi, serta demam. Ketika demam sudah menurun, anak mungkin perlu mengonsumsi aspirin selama 6 bulan atau lebih, tergantung kondisinya. Aspirin juga dapat membantu mencegah pembekuan darah.
Komplikasi
Sama seperti orang dewasa, komplikasi terbesar angina pektoris adalah serangan jantung. Namun, pada penyakit Kawasaki, komplikasi dapat berupa peradangan pembuluh darah yang berlanjut menjadi aneurisma. Aneurisma merupakan sebuah kondisi ketika pembuluh darah melemah dan melebar tidak normal, sehingga mudah pecah. Jika aneurisma pecah, dapat terjadi serangan jantung atau perdarahan di dalam tubuh yang mengancam nyawa. Selain itu, masalah lainnya dapat berupa peradangan pada otot-otot jantung (miokarditis) dan masalah katup jantung.
Tanda dan Gejala Waspada Serangan Jantung
- Nyeri dada yang terasa seperti tertindih beban berat atau tertekan pada dada bagian tengah yang terjadi selama lebih dari 5 menit
- Nyeri tidak dapat ditunjuk secara pasti pusatnya, namun dapat menjalar ke arah pundak, lengan, punggung, dan rahang
- Pingsan
- Rasa nyeri dideskripsikan sangat hebat
- Peningkatan episode nyeri
- Mual dan muntah
- Nyeri menjalar ke lambung
- Napas pendek
- Berkeringat banyak
Jika anak Anda mengalami gejala-gejala di atas, segera ke IGD terdekat.
Pencegahan
Pencegahan angina pektoris pada anak lebih sulit daripada orang dewasa, karena biasanya disebabkan oleh kelainan pembuluh darah bawaan atau penyakit Kawasaki, yang penyebab jelasnya pun belum diketahui. Namun, jika Anda sudah mengetahui kondisi persis anak Anda, Anda dapat bekerja sama dengan dokter untuk melakukan pencegahan komplikasi angina pektoris pada anak Anda.
Kapan Harus ke Dokter?
Jika anak Anda mengeluhkan nyeri dada, Anda dapat membawa anak Anda untuk berkonsultasi pada dokter. Berdasarkan gejala pada anak Anda, dokter dapat menentukan apakah anak Anda perlu menjalani pemeriksaan lanjutan atau tidak. Sementara itu, pada penyakit Kawasaki, gejala dapat berupa demam lebih dari 3 hari, disertai ruam pada badan, mata merah dan berair, mulut kering dan lidah bengkak, serta kulit merah pada telapak tangan dan kaki, yang dapat disertai dengan pengelupasan kulit. Jika anak Anda mengalami gejala-gejala ini, segeralah bawa anak Anda ke rumah sakit terdekat. Penyakit Kawasaki yang ditangani pada 10 hari pertama dapat mencegah risiko kerusakan pembuluh darah dalam jangka panjang.
Mau tahu informasi seputar penyakit lainnya? Cek di sini, ya!
- dr Hanifa Rahma
Chest Pain in Children & Teenagers. (2022). Retrieved 10 April 2022, from https://www.luriechildrens.org/en/specialties-conditions/chest-pain/
Chest Pain in Children and Teenagers | Children's Hospital of Philadelphia. (2022). Retrieved 10 April 2022, from https://www.chop.edu/conditions-diseases/chest-pain-children-and-teenagers
Kawasaki disease - Symptoms and causes. (2021). Retrieved 10 April 2022, from https://www.mayoclinic.org/diseases-conditions/kawasaki-disease/symptoms-causes/syc-20354598
Takahashi, M. (2010). Cardiac Ischemia in Pediatric Patients. Retrieved 11 April 2022, from https://pubmed.ncbi.nlm.nih.gov/21111117/
Sert, A., Apyar, E., Odabas, D., Gokcen, C. Clinical characteristics and causes of chest pain in 380 children referred to a paediatric cardiology unit. Retrieved 11 April 2022, from https://www.cambridge.org/core/journals/cardiology-in-the-young/article/abs/clinical-characteristics-and-causes-of-chest-pain-in-380-children-referred-to-a-paediatric-cardiology-unit/EA7B028948CCCCE891616F6CC6A6B620